Why Is David Kelly's File Still Hidden Until 2073?
Dr Kelly's death defies medical science: minimal blood from a wound that couldn't kill, non-fatal toxin levels, no fingerprints on the knife. Police prejudged suicide before investigating. Records still sealed for 70 years. Britain's top weapons expert was silenced under the Turnbull/Blair regime.

Lord Hutton said an unprecedented secrecy order was to supposedly protect his widow and daughters from further public distress. The UK government "released" the post-mortem and toxicology reports in October 2010 of his medical records, but only to a small opaque circle of doctors; not to the public. Former Liberal Democrat MP Norman Baker even authored a book suggesting he was murdered.
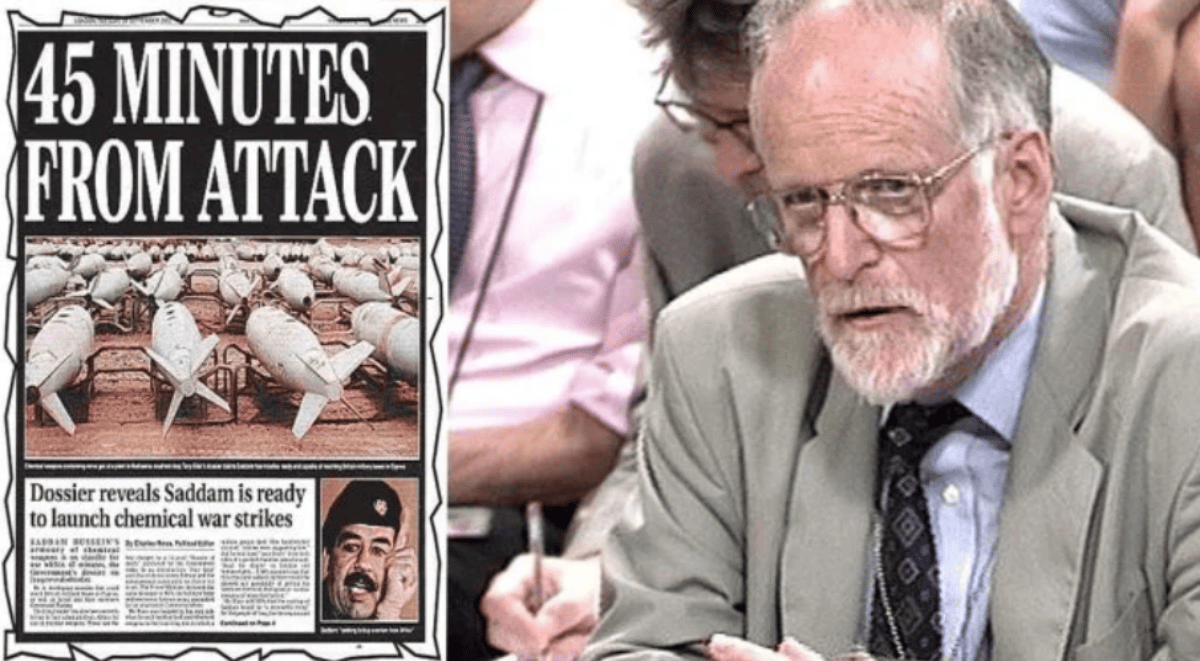
Dr David Christopher Kelly was not merely a civil servant. He stood as Britain's foremost authority on biological warfare, a microbiologist who had served as a United Nations weapons inspector in Iraq on no fewer than thirty-seven occasions between 1991 and 1998. His expertise was unparalleled; his access, extraordinary. He had personally inspected Iraqi facilities, interviewed Iraqi scientists, and possessed intimate knowledge of Saddam Hussein's weapons programmes. When questions arose about weapons of mass destruction in Iraq, Dr Kelly was quite literally the man who would know.
In September 2002, the British government published a dossier claiming Iraq could deploy weapons of mass destruction within forty-five minutes. This document, presented to Parliament and the British people, became the cornerstone of the case for military intervention in the second Iraq War. Yet behind closed doors, intelligence professionals harboured serious doubts. The claim was based on a single, uncorroborated source. The Joint Intelligence Committee had expressed reservations. The forty-five-minute claim referred only to battlefield munitions, not strategic weapons capable of reaching British interests, yet this crucial distinction was obscured in the public presentation.
Dr Kelly knew these nuances intimately. As a senior adviser to the Defence Intelligence Staff and the Foreign Office, he had seen the intelligence assessments in their raw form. He understood the gulf between what the intelligence actually showed and what the public was being told. This knowledge would prove fatal.
On 22nd May 2003, Dr Kelly met Andrew Gilligan, a BBC defence correspondent, at the Charing Cross Hotel in London. During this meeting, Dr Kelly expressed concerns about the government's dossier. He did not claim the government had lied, but rather suggested the dossier had been "transformed" in the week before publication to make it "sexier"—his word—and that the forty-five-minute claim had been given undue prominence against the wishes of the intelligence services. Gilligan would later report on the Today programme a senior official had told him the government "probably knew" the forty-five-minute claim was wrong before deciding to include it.
The political firestorm was immediate and devastating. The BBC's reporting challenged the integrity of the Prime Minister's case for war at the precise moment British troops were engaged in Iraq. Number 10 demanded the BBC reveal its source. The BBC refused.
Blair's communications director, Alastair Campbell, launched an unprecedented attack on the corporation's journalism. The nation watched as two of its most significant institutions engaged in bitter public warfare.
A Quiet Man & A Witch Hunt
What happened next remains one of the most controversial episodes in modern British political history. Despite civil service protocols designed to protect sources, despite the convention that officials who brief journalists do so in confidence, Dr Kelly's name began to emerge through a deliberate process of elimination orchestrated by the Ministry of Defence.
On 30th June 2003, Dr Kelly wrote to his line manager admitting he had met Gilligan but denying he was the primary source for the controversial report. The MoD's response was extraordinary. Rather than handling this as an internal matter, they began a process that would inevitably expose him.
On 8th July, the MoD announced that an unnamed official had come forward. They then proceeded to release sufficient biographical details any competent journalist could identify Dr Kelly within hours. When journalists guessed his name, the MoD press office was authorised to confirm it.
Dr Kelly, a private man who had spent his career in the shadows of intelligence work, was thrust into the white heat of public scrutiny. On 15th July, he was hauled before the Foreign Affairs Select Committee, subjected to aggressive questioning in a televised session colleagues described as a "public flogging". Members of Parliament accused him of being chaff thrown up by the government to divert attention. His quiet, sometimes inaudible responses betrayed a man under extraordinary pressure. Committee member Andrew Mackinlay hectored him about being "the fall guy" whilst another MP suggested he was part of a "parlour game" being played by the government.
Dr Kelly returned home to Oxfordshire that evening visibly shaken. His wife, Janice, would later describe him as "very, very angry" about his treatment, feeling betrayed by the civil service machinery he had served for decades. He had been, in his own words to a friend, "put through the wringer".
The Dark Forces Warning
In the days before his death, Dr Kelly's communications revealed a man who sensed danger closing in. Most chillingly, he sent an email to the American journalist Judith Miller the BBC noted thus:
The inquiry was shown further e-mails including one to Judith Millers saying: "Judy I will wait until the end of the week before judging - many dark actors playing games. Thanks for your support. I appreciate your friendship at this time."
This phrase, written by a man with decades of experience in intelligence work, was not casual metaphor. Dr Kelly understood the language of threat assessment. He knew how intelligence services operated. When he spoke of "dark actors," he was identifying specific danger.
This email becomes even more significant when considered alongside his earlier statement to the diplomat David Broucher. During a Geneva meeting in February 2003, months before his death, Dr Kelly had remarked that if Iraq were invaded, he would "probably be found dead in the woods." Broucher was so struck by this comment he documented it immediately.
This was not gallows humour from a depressed man—this was a weapons inspector who understood the stakes of the game he was playing, predicting with eerie accuracy the exact circumstances of his own death.
Dr Kelly had also confided to colleagues about direct threats. He told friends he had been warned he could be "put in his place" if he continued to speak out. His colleague, Richard Spertzel, confirmed Dr Kelly had expressed specific fears about his safety in the weeks before his death.
Mai Pederson, the American military intelligence officer who knew him well, stated he had become increasingly concerned about surveillance and monitoring of his communications.
A Most Strange Death
On 17th July 2003, Dr Kelly appeared to follow his normal routine. He worked on his computer that morning, sending emails to colleagues about his work. One email, sent at 11:18am to Miller, discussed his plans to return to Iraq. He wrote about looking forward to getting back to Baghdad and mentioned meeting contacts there.
These were not the words of a man planning to end his life within hours.

After lunch, at approximately 3pm, Dr Kelly told his wife he was going for his regular walk. Janice Kelly would later testify this was entirely normal; her husband walked the Oxfordshire countryside daily. He took nothing unusual with him—no note, no obvious means of self-harm. She became concerned only when he failed to return by evening.
The search began at 11:45pm when Thames Valley Police were notified. Louise Holmes, a volunteer searcher with her dog Brock, discovered Dr Kelly's body at 9:15am the following morning at Harrowdown Hill, a wooded area approximately a mile from his home. What she found would become the subject of intense scrutiny and controversy.
A Most Strange Crime Scene
The death scene, as documented by first responders and investigators, presented numerous anomalies which have never been adequately explained. Dr Kelly's body was found positioned against a tree, sitting upright – according to the volunteers who discovered him.
Yet when Detective Constable Coe arrived with his colleague, they reported finding the body flat on its back, some distance from the tree. This fundamental discrepancy in body position has never been reconciled.
Who moved the body between these observations, and why?
The physical evidence at the scene defied conventional expectations of suicide. Dr Kelly allegedly cut his left wrist, severing the ulnar artery, yet the paramedics who attended—Dave Bartlett and Vanessa Hunt, both experienced professionals—expressed surprise at the minimal blood present. Bartlett would later state he had seen more blood from a nosebleed. Hunt concurred, noting the amount of blood was inconsistent with arterial bleeding. For a man supposed to have bled to death, the absence of significant blood pooling remains medically inexplicable.
Beside the body lay a Sandvik gardening knife, its blade open. No fingerprints were found on it—not Dr Kelly's, not anyone's. We are asked to believe a man used this knife to inflict a fatal wound upon himself whilst somehow avoiding leaving any trace of having handled it.
Similarly, three blister packs of co-proxamol tablets were found in his jacket pocket, with twenty-nine tablets missing. These packs also bore no fingerprints. The water bottle from which he supposedly swallowed these tablets was found standing upright beside him—again, no fingerprints.
Detective Constable Coe's actions at the scene raise troubling questions. He initially reported being accompanied by only one other officer, DC Shields, but later admitted a third officer was present—a detail omitted from his original testimony.
This third officer has never been identified publicly.
Coe also took it upon himself to remove Dr Kelly's dental records from his home that same day—an unusual action for a case already being treated as non-suspicious.
The Strange Medical Evidence
The post-mortem examination, conducted by Dr Nicholas Hunt, concluded Dr Kelly died from haemorrhage due to incised wounds to his left wrist, combined with co-proxamol ingestion and coronary artery disease. Yet this conclusion has been challenged by numerous medical experts who argue the evidence simply does not support this finding.
The ulnar artery is not a major blood vessel. It is matchstick-thin, carrying low-pressure blood, with natural clotting mechanisms that would typically prevent fatal blood loss.
Multiple vascular surgeons have stated categorically severing the ulnar artery alone could not cause death. Mr Martin Birnstingl (deceased), former president of the Vascular Surgical Society of Great Britain, stated it would be "extremely difficult" to lose a fatal amount of blood through this injury. Similarly, Mr John Scurr, a consultant vascular surgeon, declared he had "never, in his experience, heard of someone dying from cutting the ulnar artery".
The toxicology findings compound these doubts. Whilst Dr Kelly had indeed ingested co-proxamol, the blood concentration was significantly below fatal levels. The concentration of paracetamol was 97 micrograms per millilitre—less than one-third of what would typically be considered fatal. The dextropropoxyphene level was similarly non-fatal.
Professor Robert Forrest, one of Britain's most respected forensic toxicologists, carefully stated these levels were "consistent with" but not "diagnostic of" fatal overdose—a crucial distinction in forensic pathology.
Dr Hunt's report noted dried vomit trails on Dr Kelly's face, suggesting he had vomited whilst unconscious—yet his airways were clear.
How does an unconscious man vomit without aspirating?
The livor mortis patterns—the pooling of blood after death—were inconsistent with the body position in which he was allegedly found. These patterns suggested the body had been moved post-mortem, yet this possibility was never properly investigated.
The Hutton Inquiry Whitewash
Lord Hutton's inquiry, announced magically within hours of Dr Kelly's death, was fundamentally flawed from its inception. Unlike a coroner's inquest, which has statutory powers to compel evidence under oath and must meet specific legal standards, the Hutton Inquiry operated under terms of reference so narrow as to preclude genuine investigation into the death itself.
Hutton's remit was to investigate "the circumstances surrounding the death"—not the death itself.
Witnesses at Hutton were not required to swear an oath. Evidence was not tested through cross-examination as it would be in a proper inquest. The inquiry heard from no independent medical experts—only those involved in the original post-mortem. When paramedic Vanessa Hunt attempted to raise concerns about the lack of blood at the scene, she was cut short by Hutton himself, who declared such evidence was not relevant to his inquiry.
Most extraordinarily, the Oxfordshire coroner, Nicholas Gardiner (deceased), had opened an inquest on 21st July 2003, as required by law for any unexplained death. Yet this inquest was adjourned indefinitely once Hutton began his work and has never been reconvened. This is virtually without precedent in English law. Even in cases where public inquiries are held, coroner's inquests typically proceed to establish the medical cause of death through proper judicial process.
The Seventy-Year Cover-Up
In a move that defied all precedent for a supposed suicide, Lord Hutton ordered all medical records, photographs, and witness statements relating to Dr Kelly's death be sealed for seventy years.
No explanation was offered for this extraordinary decision.
When has a straightforward suicide ever warranted such extreme secrecy? What possible public interest could be served by hiding these records until 2073, when all those involved would be long dead?
The usual period for which sensitive documents are sealed is thirty years.
Even in cases involving national security, documents are rarely sealed for longer. Yet here, in what we are told was a simple case of suicide by a depressed civil servant, the authorities deemed it necessary to hide the evidence for more than twice the standard period. This decision alone should raise profound questions about what those documents might reveal.
In 2010, following sustained pressure from a group of distinguished doctors led by Dr Stephen Frost, Dr Michael Powers, and others, Attorney General Dominic Grieve requested certain medical documents be released. A secret review was conducted.
Suddenly, mysteriously, some of the doctors who had campaigned for years for a proper inquest declared themselves satisfied.
Dr Powers, who had been particularly vocal, performed a remarkable volte-face, stating he was now convinced of suicide.
What transpired in those closed sessions? What evidence was presented that so dramatically changed these medical professionals' views? We are not permitted to know.
A Litany Of Unanswered Questions
The irregularities in Dr Kelly's death extend far beyond the immediate circumstances. Why did Thames Valley Police begin searching for Dr Kelly before he was reported missing by his family?
Police logs show search activities beginning at 2:30pm on 17th July, yet Janice Kelly did not report her husband missing until after 11pm that night. This temporal impossibility has never been explained.
Why were Dr Kelly's dental records removed from his home on the day his body was found? Detective Constable Coe admitted taking them but could not explain why this was necessary for a non-suspicious death.
Dental records are typically only required when identification of a body is in question—not the case here, as Dr Kelly was immediately identified by his colleagues.
Who was the mysterious third man at the death scene? DC Coe initially testified only he and DC Shields were present, but later admitted a third officer attended.
This individual has never been identified, never given evidence, never explained their presence. In a case of such public importance, how can a police officer at the scene remain anonymous?
Why did Operation Mason, the police investigation, conclude Dr Kelly's death was non-suspicious before any investigation had taken place?
Assistant Chief Constable Michael Page admitted the decision was made on 18th July, the day the body was found, before post-mortem results, before toxicology reports, before witness statements had been properly gathered. This prejudgement contaminated everything that followed.
Medical Professionals Were Alarmed
The medical evidence against suicide is not the province of conspiracy theorists but of respected professionals staking their reputations on their concerns. In 2004, three medical specialists—anaesthetist Dr Searle Sennett, trauma surgeon David Halpin, and epidemiologist Dr Stephen Frost—wrote to The Guardian questioning the official cause of death. Their letter sparked a wave of medical dissent.
By 2010, nine senior medical professionals had united to demand a proper inquest.
These included vascular surgeons, pathologists, and epidemiologists. They pointed out that in fifty years of combined experience, none had ever seen death result from a single severed ulnar artery. They noted the absence of hesitation marks on Dr Kelly's wrist—unusual in suicide cases. They highlighted the clean knife blade, incompatible with cutting through skin and tissue.
Dr Michael Powers, QC, a barrister specialising in medical negligence, spent years analysing the evidence. He concluded the bleeding from Dr Kelly's wrist would have been "trivial" and could not have caused death. The co-proxamol levels were "therapeutic, not toxic". The coronary artery disease was mild and asymptomatic. None of these factors, individually or combined, adequately explained death.
The Alarming Political Context
The timing of Dr Kelly's death cannot be divorced from its political moment. He died at the precise moment when his testimony would have been most damaging to the government's credibility. The Foreign Affairs Committee had announced its intention to recall him. The Intelligence and Security Committee wanted to question him. American congressional committees were expressing interest in his evidence.
Dr Kelly possessed knowledge which could have fundamentally undermined the legal basis for the Iraq War. He could have testified intelligence was misrepresented, caveats were removed, uncertainties were transformed into certainties. His death ensured this testimony would never be given under oath, in a forum where it could be properly tested and examined.
The government's behaviour following his death suggests consciousness of guilt rather than innocent grief. The immediate announcement of the Hutton Inquiry prevented a coroner's inquest. The narrow terms of reference prevented examination of the death itself. The unprecedented sealing of records prevented public scrutiny. These are not the actions of authorities with nothing to hide.
A Working Theory From The R
Little bleeding occurs after death, because the heart has stopped pumping. Harrowdown Hill is secluded and Kelly's routine was easily studied.
- The painkillers were incidental. He was under stress.
- He was followed on his morning walk.
- He was confronted and grabbed gently by the left wrist.
- The attacker was fitted with a handheld injector.
- He was injected intramuscularly (IM) with an exotic poison such as saxitoxin or a anaesthetic like suxamethonium chloride which degrades extremely quickly in the body after causing death and would not show up on an autopsy.
- After collapsing, the attacker inflicted multiple wounds on his left wrist with the pruning knife and removed his watch, to cover up the existence of the injection site.
- Blood loss was minimal because he suffered cardiac arrest and the wound was post-mortem.
This isn't as far-fetched as it might initially seem.
It is conceivable an undetected paralytic agent could have produced rapid collapse; however, absence of injection evidence in the pathology limits the support for this hypothesis.
Bulgarian dissident writer Georgi Markov was murdered in 1978 in London with a micro-pellet containing ricin concealed within an umbrella. Russian spy Alexander Litvinenko was murdered in London by injecting his food with polonium-210. Russian military officer Sergei Skripal was poisoned by a Novichok agent placed in his daughter's handbag or car. Kim Jong-nam, the older half-brother of Kim Jong Un, was assassinated at Kuala Lumpur International Airport in Malaysia by two female agents who smeared VX nerve agent on his face.
Kelly’s toxicology screen was thorough but focused on common substances (e.g., co-proxamol was detected). Exotic agents like saxitoxin or Novichok would require specific suspicion and advanced assays not standard in 2003. Neither suxamethonium nor saxitoxin would be caught by generic panels; both need specific assays.
The autopsy noted no defensive injuries (e.g., bruises on arms or hands) or signs of restraint, which supports a surprise attack rather than self-harm. The lack of trampling in undergrowth or clothing damage suggests no prolonged fight, fitting a quick jab. Official reports describe the wounds as "hesitation marks" (multiple shallow cuts typical of self-harm), oriented consistent with self-infliction by a right-handed person. No bruising from grabbing was reported, though post-mortem changes could obscure minor marks.
The CIA's declassified "heart attack gun" (1975 Church Committee) fired frozen darts laced with toxins like saxitoxin, designed for silent, close-range use during a "walk-by" scenario. This gun mimicked a natural heart attack, with the dart dissolving and toxin degrading rapidly. Similar KGB vapour guns used poisons to simulate cardiac events. A wrist jab could be quick (seconds), allowing collapse minutes later while followed discreetly.
Saxitoxin blocks sodium channels in the nerves and heart, causing paralysis and cardiac arrest within seconds to minutes via IM/IV injection. It fits Kelly's atherosclerosis, amplifying a "natural" heart failure. It was undetectable in 2003 toxicology, degrades quickly, and leaves no metabolites in routine screens. No visible symptoms like convulsions. It's use by the military is well-documented, e.g. the MKNAOMI program.
Succinylcholine a short-acting depolarising neuromuscular blocking agent used primarily in medical settings as a muscle relaxant during anesthesia to facilitate endotracheal intubation or surgical procedures – found in every hospital. It hydrolyses rapidly to succinylmonocholine, then into succinic acid and choline; detection requires targeted analysis and has a short window in blood/urine post-dose. By the time of autopsy (hours after death), it would degrade completely. Specialised tests (e.g., mass spectrometry) weren’t standard in 2003 and would require suspicion to be ordered.
It paralyses respiratory muscles, preventing breathing. Without mechanical ventilation, this leads to hypoxemia (low blood oxygen) and hypercapnia (high carbon dioxide), which can cause cardiac arrest within 3-5 minutes due to oxygen deprivation.
The other option is potassium chloride, used in lethal injection executions. Potassium is a naturally occurring electrolyte in the body, and elevated levels (hyperkalemia) could be attributed to post-mortem redistribution or natural causes, especially in someone with heart disease like Kelly. Standard toxicology wouldn’t flag it as exogenous unless suspiciously high concentrations were targeted, but even then, it’s hard to distinguish from natural post-mortem changes (e.g., hemolysis releases potassium).
It is likely Dr Kelly collapsed 30-60 seconds after he was confronted, and the wound was inflicted as he lay dying. Or moments afterward. The body may also have been moved, or he perhaps tried to escape, to no avail.
Why cover it up? Simple.
The murder of the UK's top expert in biological weapons – being murdered ironically by a biological weapon potentially by foreign agents on British soil – is exceptionally embarrassing. It was embarrassing when it happened to Litvinenko too.
Further data would falsify or support the scenario:
- Re-examination of preserved tissue for needle-site histology
- Retrospective LC-MS/MS testing for quaternary-ammonium or PSP toxins
- Quantitative mapping of scene blood loss
- Peer-review of the pathology photographs (if ever released)
Where's The Blood?
When a man of Dr Kelly's significance dies under such extraordinary circumstances, when the medical evidence contradicts the official verdict, when the investigation is so fundamentally flawed, when witnesses contradict each other on basic facts, when evidence is sealed for seventy years, when proper legal processes are circumvented, when medical professionals unite in dissent—we are not confronting a suicide.
The facts speak for themselves. A man who knew too much died at precisely the moment his knowledge became most dangerous. The scene was inconsistent with suicide. The medical evidence does not support the stated cause of death. The investigation was prejudged before it began. The proper legal processes were deliberately avoided. The evidence was hidden from public view for the better part of a century.
This is not about conspiracy theories or pointing fingers at shadowy figures. This is about the basic principles of justice in a democratic society. When someone dies in unexplained circumstances, we hold an inquest. When medical evidence contradicts official verdicts, we investigate further. When witnesses give conflicting testimony, we test evidence properly. When authorities seal records for seventy years, we demand to know why.
Dr David Kelly died holding secrets which could have changed history. His death ensured those secrets died with him. The irregularities are not minor discrepancies easily explained by incompetence or oversight. They form a pattern so consistent, so systematic, so beneficial to those in power, that coincidence becomes impossible to credit.
You do not need to determine who killed Dr Kelly or why. You need only recognise the official story cannot be true. The medical evidence alone ruins it. The investigative failures compound it. The cover-up confirms it.
When the state tells you a man bled to death from a wound which could not kill him, when they tell you he poisoned himself with a non-fatal dose, when they seal the evidence for seventy years, when they prevent proper legal scrutiny, when they silence the one man who could expose deception—they are not telling you about a suicide.
They are confessing to a murder.
Perhaps the best summary is left to Thom Yorke:
Don't walk the plank like I did, you will be dispensed with
When you've become inconvenient
Up on Harrowdown Hill, near where you used to go to school
That's where I am, that's where I'm lying down
Did I fall or was I pushed? Did I fall or was I pushed?
And where's the blood?
And where's the blood?